
INTERPROXIMAL REDUCTION
Often it will be important to create some space so teeth can be moved into a more ideal position. The three main ways traditionally to achieve this are:
1.Expansion or Arch Development
2.Extraction
3.IPR Interproximal Reduction or some times known as “Stripping”
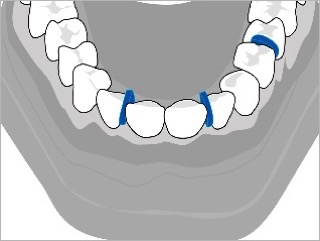
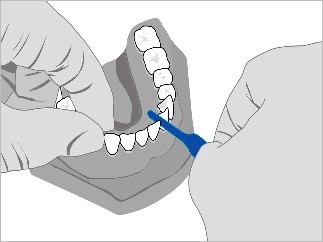
This image shows the use of orthodontic separators prior to IPR
The Truline system can use all three methods to achieve space but expansion and IPR are the most common.
The use of IPR has been well documented, it was first described by Ballard in 1944 and is one of the most conservative methods available to alleviate crowding.
In addition to creating space, IPR flattens the contact areas, which can increase the stability of the final result. This helps minimize relapse after treatment.
IPR can be performed at any time during the treatment, whenever more space is needed.

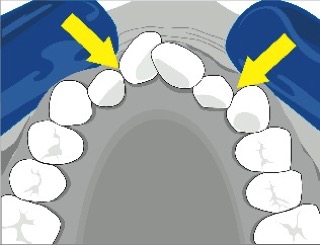
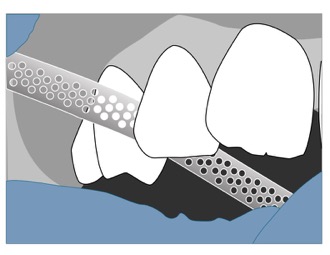
This image shows the use of a diamond disk for IPR
In addition to creating space, IPR also reduces the friction between tooth contacts; this reduces the amount of resistance the Truline aligners must overcome thus allowing for quicker tooth movement.
There are many ways to perform IPR, including the use of diamond disks, diamond strips, or diamond and carbide burs. Many have found the most rapid and effective way to perform IPR is to begin with a diamond disk followed by smoothing and cosmetic recontouring of the tooth with a finishing bur. A diamond strip, or interproximal finishing strip, can then be used for final finishing of the interproximal enamel, if desired. When completed, the tooth morphology should not have changed significantly. The tooth should look like a slightly smaller version of its previous self. This method quickly, safely and efficiently creates space to move the teeth.
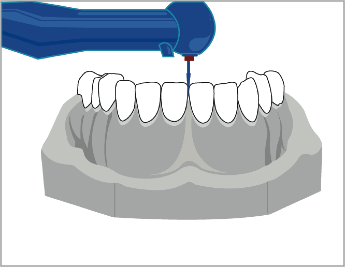
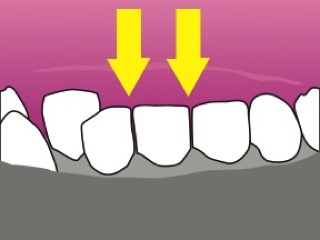
This image shows an example of only using a disk where the contacts are well aligned
Sheridan suggested that 50% of the interproximal enamel could be reduced. Proffit says the teeth can be reduced up to 0.5mm on each side without reaching the dentin. Research has found that often you can IPR more than 0.5mm, especially on wide teeth, with no adverse effects.
A significant amount of space can be gained by IPR. For example, if you IPR all the contacts from the distal of #6 to the distal of #11 you can often gain from 5 to 7 mm of space. This is usually more than enough to correct crowding in most cases.
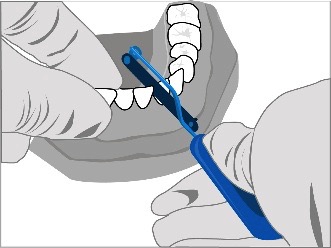
This image shows a diamond bur for IPR
Sheridan suggested that 50% of the interproximal enamel could be reduced. Proffit says the teeth can be reduced up to 0.5mm on each side without reaching the dentin. Research has found that often you can IPR more than 0.5mm, especially on wide teeth, with no adverse effects.
A significant amount of space can be gained by IPR. For example, if you IPR all the contacts from the distal of #6 to the distal of #11 you can often gain from 5 to 7 mm of space. This is usually more than enough to correct crowding in most cases.
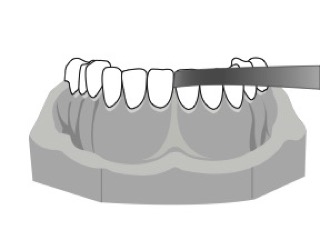
This image shows a diamond file for IPR
This image shows a feeler guage used to measure IPR amount
Is IPR safe?
Although you can use IPR anywhere we need space, it seems IPR should be used where the enamel is thickest.
On the upper anterior teeth, the thickest enamel is on the mesial and distal of the canines and the distal surfaces of the central incisors. On the lower anterior teeth, the thickest enamel is on the mesial and distal surfaces of the canines and the distal surfaces of the lateral incisors. Many doctors are concerned that the thinning of enamel will increase the patient’s susceptibility to tooth decay and periodontal disease.
In actuality investigators have reported no increase in either caries or periodontal disease due to a reduced enamel surface. Sheridan stated that no study indicated how much enamel is needed for adequate protection of the teeth.
The natural variation in thickness of enamel suggests that there is no protective advantage in preserving thick interproximal enamel when thin enamel occurs naturally on the facial and lingual surfaces of the teeth. Some studies did show some increased roughness of IPRed enamel when compared to virgin enamel, but there was no increase in decay. In one study El-Mangoury indicated that IPR did not expose enamel to changes that caused caries. There was a period of demineralization followed by remineralization within nine months. Some have suggested placing a sealant after IPR, but this would actually interfere with the constant remineralization that naturally occurs. However, a fluoride treatment can be given after IPR.
Craine and Sheridan also demonstrated that IPR'ed teeth are no more susceptible to caries or periodontal disease than unaltered surfaces. When done properly IPR has no negative effects on the bone or interproximal tissue. Tuverson reported a negligible periodontal change and showed gingival papillae that were actually greatly improved after correcting crowding with IPR. In a nine year study Boese found no significant increase in pocket depth, gingival recession or loss of alveolar bone.Is IPR safe?
Although you can use IPR anywhere we need space, it seems IPR should be used where the enamel is thickest.
On the upper anterior teeth, the thickest enamel is on the mesial and distal of the canines and the distal surfaces of the central incisors. On the lower anterior teeth, the thickest enamel is on the mesial and distal surfaces of the canines and the distal surfaces of the lateral incisors. Many doctors are concerned that the thinning of enamel will increase the patient’s susceptibility to tooth decay and periodontal disease.
In actuality investigators have reported no increase in either caries or periodontal disease due to a reduced enamel surface. Sheridan stated that no study indicated how much enamel is needed for adequate protection of the teeth.
The natural variation in thickness of enamel suggests that there is no protective advantage in preserving thick interproximal enamel when thin enamel occurs naturally on the facial and lingual surfaces of the teeth. Some studies did show some increased roughness of IPRed enamel when compared to virgin enamel, but there was no increase in decay. In one study El-Mangoury indicated that IPR did not expose enamel to changes that caused caries. There was a period of demineralization followed by remineralization within nine months. Some have suggested placing a sealant after IPR, but this would actually interfere with the constant remineralization that naturally occurs. However, a fluoride treatment can be given after IPR.
Craine and Sheridan also demonstrated that IPRed teeth are no more susceptible to caries or periodontal disease than unaltered surfaces. When done properly IPR has no negative effects on the bone or interproximal tissue. Tuverson reported a negligible periodontal change and showed gingival papillae that were actually greatly improved after correcting crowding with IPR. In a nine year study Boese found no significant increase in pocket depth, gingival recession or loss of alveolar bone.
Remember, IPR also reduces the friction between tooth contacts; this reduces the amount of resistance the Truline aligners must overcome thus allowing for quicker tooth movement. So even minimal loosening of contacts can always be beneficial.
Thanks to Dr Dr. Richard J. DePaul, Jr and Donal Inman for kind permission to use some information on this page.
